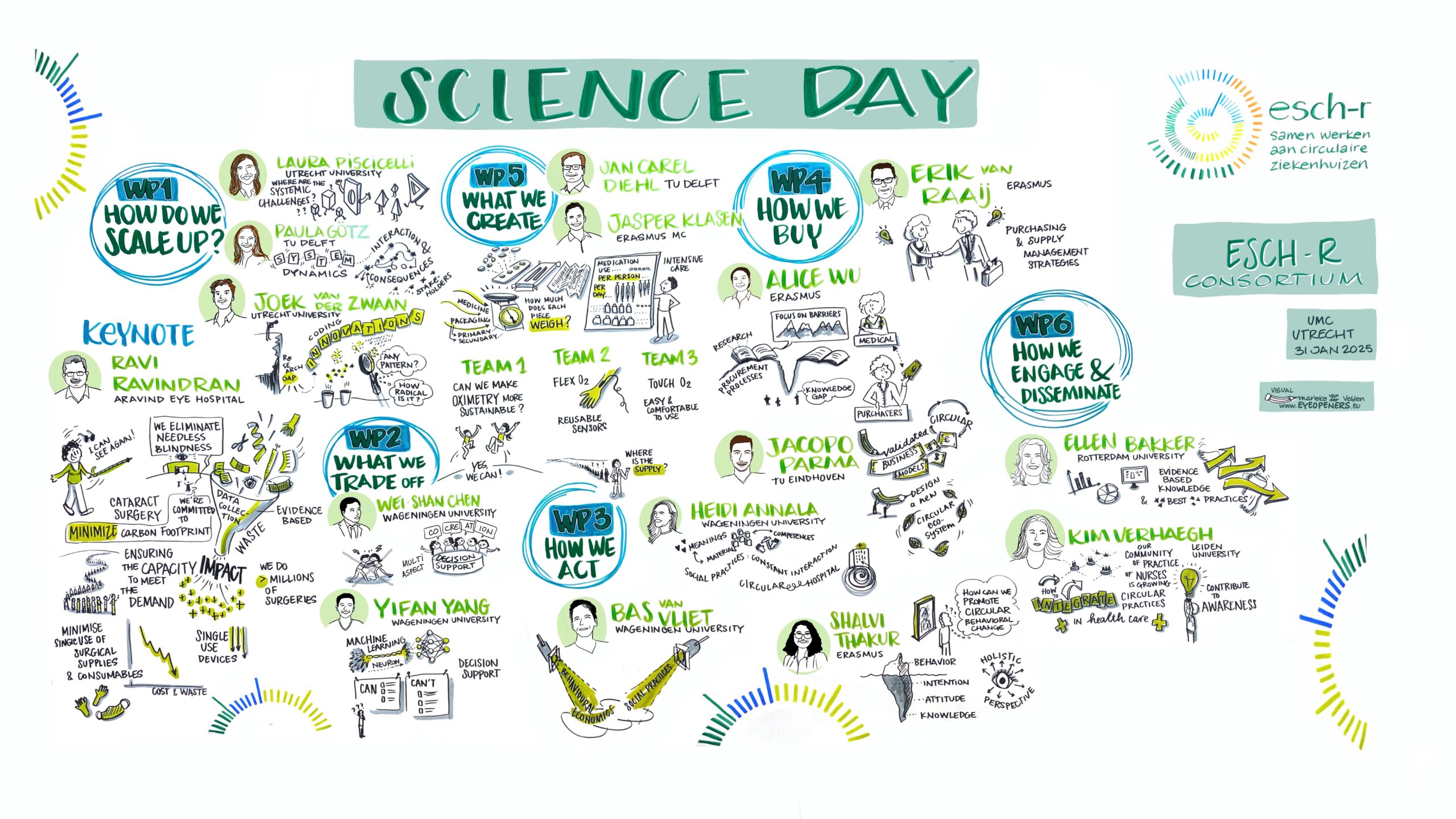
The WP leaders and their PhD’s gave an update on their efforts during the first annual ESCH-R Science Day 2025. The event was chaired by PI Nicole Hunfeld (Erasmus MC) and project board member Albert Wagelmans (Erasmus University).
Keynote speaker
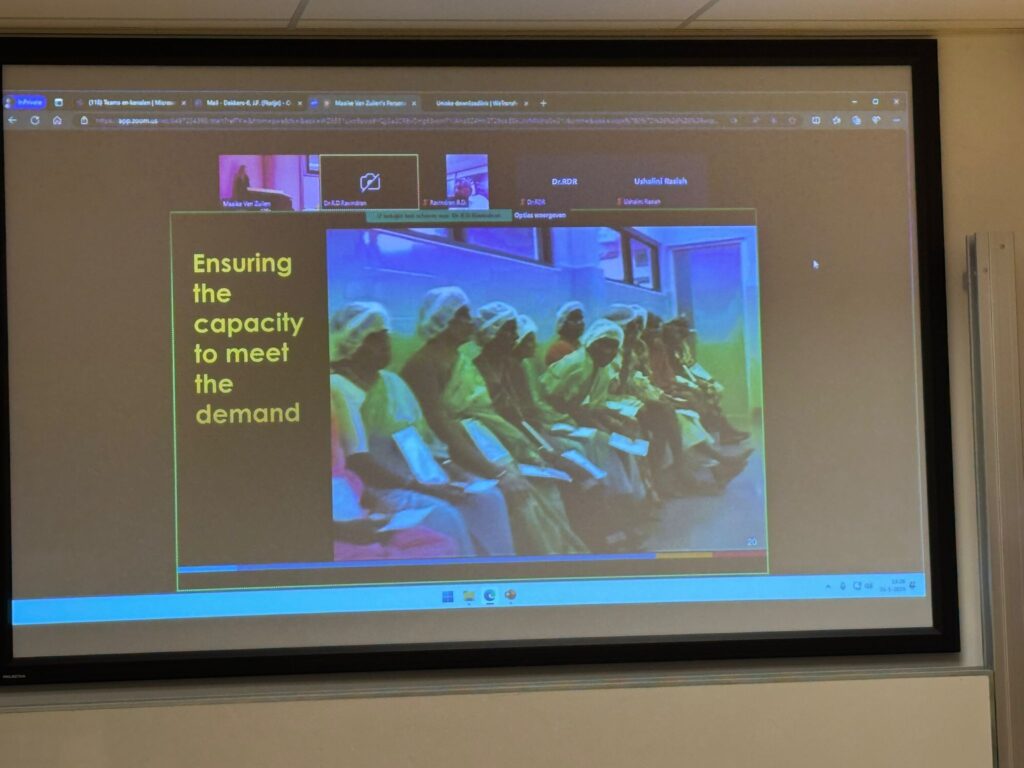
The Science Day programme kicks off with an interesting keynote by Dr Ravi Ravindran, Director Quality of the Aravind Eye Hospital in Madurai, India. The Aravind hospital group, which performs 450.000 cataract surgeries per year, produces only 5% of the amount of waste that is produced in hospitals in the Western world. One cataract surgery in the US generates the same of waste as 93 surgeries do in Aravind. And: Aravind generates about 6 kg CO2-equivalent per phaco procedure. This is only 4% of the UK’s emissions per phaco.
Dr Ravindran explains Aravind Hospital achieved this by changing their procedures. One operating team, consisting of 1 surgeon, 2 nurses and 2 technicians, perform 25 to 30 operations in one back to back session. The procedures take place in one OR with 2 patient beds, 2 surgical trolleys, a single microscope and a single phacoemulsification machine. Het team scrubs only once and wears reusable cotton gowns, which are not changed in between the operations. The nurses wear no gloves, but use antiseptic solution. And the instruments are sterilized at a high temperature during a short cycle, and are packed without individual wrapping. Also, BSS-solution is shared, the same phaco cassette and tubing is used during the whole day, and multi-use eyedrops are used.

The measures have no negative impact on hygiene. In fact, the number of infections at Aravind is significantly lower than that in the UK: 0.0170% versus 2.1%.
“Changing habits in the OR needs high level of commitment from the leadership”, advises Dr Ravindran. “It is also important to raise staff awareness and engagement. Once you identify the areas of waste, you can implement evidence based practices to reduce the carbon footprint.”
Aravind’s approach demonstrates that high-quality, high-volume cataract surgery can be both cost-effective and environmentally sustainable. The session encouraged hospitals to rethink their surgical protocols and adopt circular practices in healthcare.
Workpackage 1 – How we scale up: analyzing systemic barriers and enablers for the implementation of circular interventions in hospitals


“WP 1 team looks at what is happening and how we can make an impact by scaling up innovations for circularity”, says WP leader Laura Piscicelli (UU). “We analyze systemic barriers and enablers for circular interventions, and then come up with a roadmap for successful implementation. We want to look at the problems and how they are prioritized, and the factors that can scale up the circular interventions, also by looking at policy.”
Paula Goetz (PhD TU Delft): “In order to analyze systemic barriers and enablers for circular interventions, you need to view the system as a whole.” Paula will use the system dynamics modelling with stakeholders for this. “In a group building model we can see how different subsystems, such as hospitals and suppliers, affect each other. The method can also be used to determine uncertainties and to design interventions and their consequences.” In the coming years she intends to include the perspective of stakeholders to form a comprehensive system understanding, and to develop policy recommendations that work for all stakeholders. Storage is not the only factor that influences the use of consumables; that is why Paula will also look at other factors such as behavior and protocols.
Joek van der Zwaan (PhD UU) worked on a paper on existing circular innovations at Dutch hospitals. “Everyone focusses on new solutions, but it is also useful to look at what has already happened in the sector.” However, there was little information on this topic. “We tried to fill this gap by providing an overview of past circular innovations, and how those innovations have developed over time. Joek collected information, data, reports from hospitals. The innovation data were coded and analyzed with regards to R-strategies and value chain. In some cases, some patterns were already visible. The next step is to see if any further patterns can be detected. More data will hopefully be available soon.
Workpackage 2 – What we trade off: decision support framework prioritizing interventions
“There are many options when it comes to circular interventions, and even per individual intervention”, explains WP-leader Wei-Shan Chen (‘Momo’, WUR). “The question is: where to start, thereby also taking the limitations (money, knowledge, capacity) into consideration.” WP2 aims to create a decision support framework. The intended key output includes a database R-interventions for hospital disposables, a multi-aspect performance decision maker and optimizer, and young talents/wiser scientists.
Yifan Yang (PhD WUR) talks about AI-based data collection and MFA creation for designing circular hospitals. “With AI we try to create a smart tool which can help select interventions. WP2 wants to train the model to recognize which medical plastic products are used during the cataract surgery, in which phase and in which amount. Once this benchmark is set, interventions can be tested and evaluated. The best practices can then be tested in living labs, in cooperation with other workpackages.
“How about the CO2-footprint for AI?” Nicole Hunfeld asks. “Training an AI model does affect the environment considerably”, Yang agrees. “But once the model is ready, it can be used on a widescale basis by hospitals to become more circular.” ”On the website green-algorithms.org you can calculate the negative and positive impact”, someone from the audience advises.
Workpackage 5 – What we create: co-creation with stakeholders in living labs in medical centers
Living Labs is the topic on which WP5 focusses. In two living labs (UMCU, Erasmus MC) innovations and interventions are co-created, together with stakeholders inside and outside of the hospital. WP5 leader Jan Carel Diehl: “There are 6 different settings: IC, intervention cardiology and obstetrics in Erasmus MC, and ophthalmology, urology and nephrology in UMCU.”
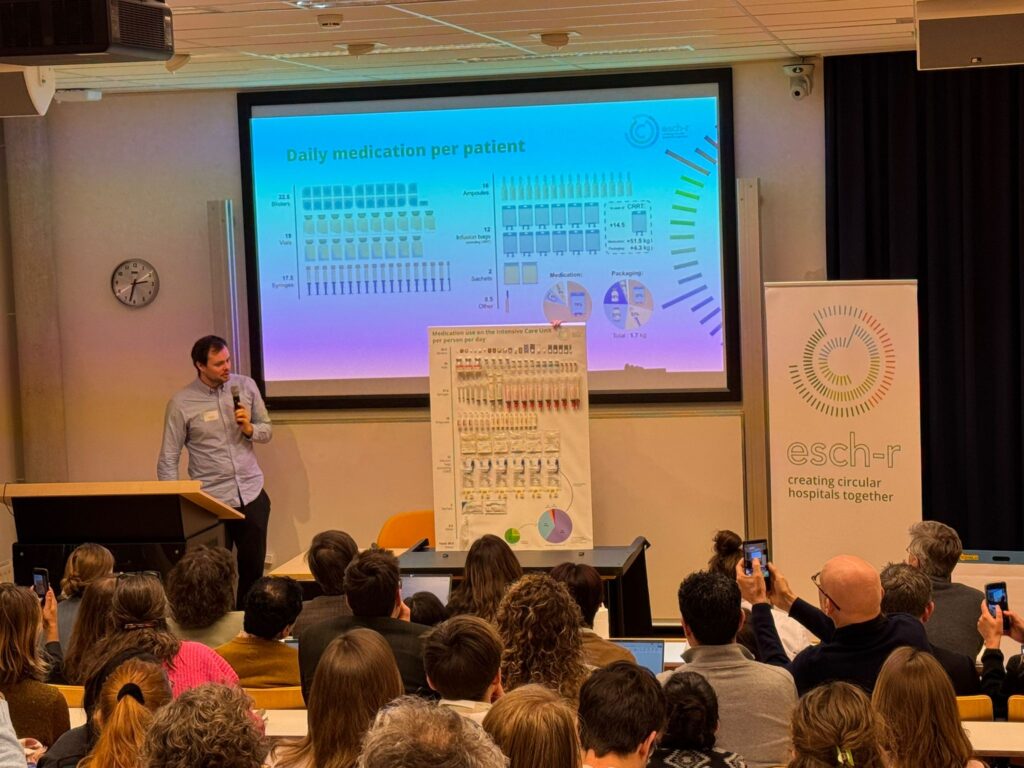
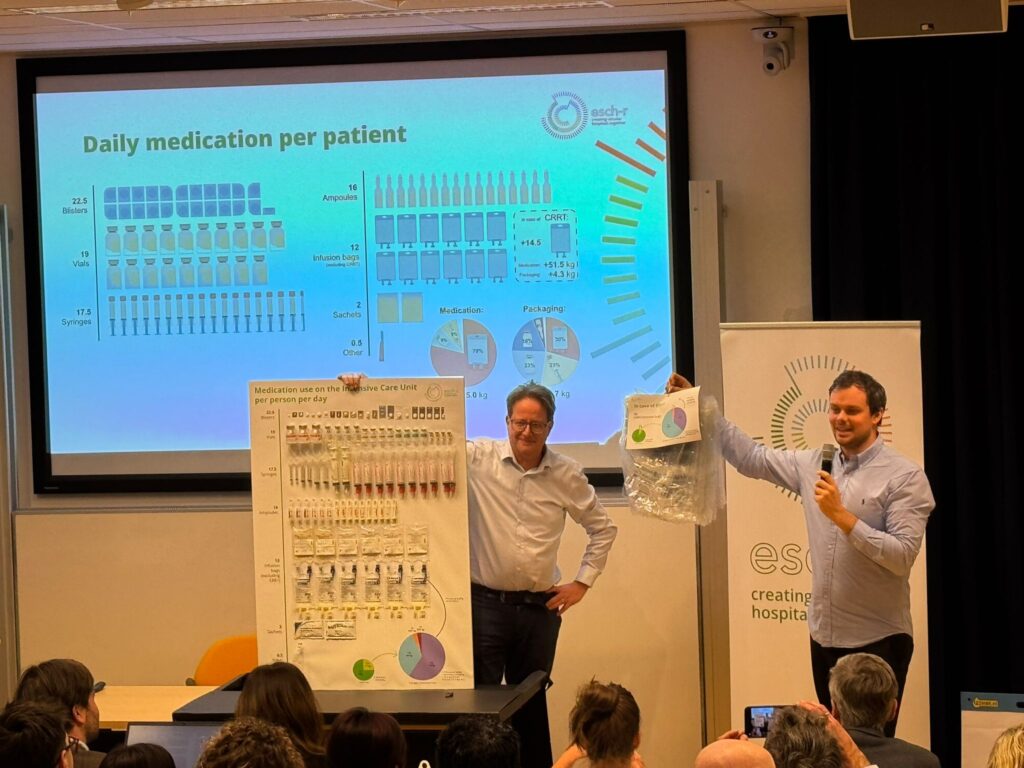
PhD Jasper Klasen (Erasmus MC) presents an update on case study 1: circular material flow of medication in the ICU. The use of medication in the ICU’s contribute to the carbon footprint significantly. Klasen conducted a Material Flow Analysis (MFA) in order to investigate which materials enter, are used in, and leave the ICU. The results are presented in a material flow chart. What stands out: the dialysis bags form the largest part of the material flow. Also: fluid medication creates much more waste mass than tablets.
As for potential sustainable interventions, Klasen advises medication-related strategies, such as to prioritize oral formulations over intravenous formulations, develop/use more concentrated fluid formulations, and use alternatives to traditional CRRT in order to minimize the use of fluids and materials.
Case study 2 is all about improving an existing medical device: the pulse oximeter. The single use varieties create a lot of waste. Three student groups came up with ways to make the device more circular. They pitch their ideas.
Emma Kockelkoren and Vera Hijlkema redesigned a reusable pulse oximeter in order to make it more desirable, so that it would be used more often. This led to the creation of DESMOS, which has an attachment point at the wrist that increases stability, comfort and reliability.
The team of Omri Steinmetz and Katie Wood created the FLEX-O2, a pulse oximeter consisting of a reusable sensor and plug, and a disposable sensor mount made of ecofriendly materials. Also, more than 2 wavelengths will be incorporated into the device. The carbon footprint of the FLEX O2 is rather high at the beginning of its lifecycle, but over time remains as low as that of reusable devices.
Laura ter Horst and Emma Rens introduce the TOUCH O2. The device consists of a cable including the electronics, a clip which converts the cables to the connector and a toggle which can be adjusted in order to fit various finger sizes. The benefits: an improved fit, which makes it comfortable to wear, also for a long time, and a CO2 reduction of 50%.
Workpackage 3 – How we act: the hospital culture and practices of care professionals on sustainable behavior
After the break, it’s time for an update of Workpackage 3, which deals with a social scientific behavioral theme. WP leader Bas van Vliet (WUR): “We are going to study existing behaviors, and the drivers and protocols behind them. The behavioral economists in our team look at the interpersonal factors that drive behavior, the sociologists focus on the social and material context of behavior. The combined information can be used to consider interventions.”
Heidi Annala (PhD Wageningen University) focusses on social practice, the external context of behavior. There are 3 components that form social practices: meanings, competences and materials. Annala researches how current practices shape and sustain the reliance on single use materials. She intends to focus on role that protocols play in this behavior, and is interested in how practices can be re-designed to make them more circular. In a living lab situation, her data will feed into those interventions.


Shalvi Thakur (PhD Erasmus University) researches the drivers and interventions to promote circular behavior. “Delivering more circular healthcare involves having knowledge and changing your attitude, intention and behavior. Many factors affect this process, such as patient safety, availability and work pressure. Behavior is just the tip of the iceberg, this should be changed. Thakur will conduct surveys in order to better understand the role of knowledge on circularity in hospitals. This will lead to the development of interventions to be tested in the hospital.
Workpackage 4 – How we buy: partnering with the supply chain to co-create circular interventions
“Our workpackage is all about the interactions between hospitals and their suppliers”, says WP leader Erik van Raaij (Erasmus University). We look at which business models for suppliers can stimulate circularity, but also what kind of purchasing strategies in hospitals can help to achieve this.

Alice Wu (PhD Erasmus University) focusses on the hospital point of view at purchasing strategies. “Procurement has a key position in the healthcare ecosystem, it determines which materials come in and how much waste comes out of the hospital.” Not much research has been done when it comes to sustainable procurement in healthcare. Wu made her own analysis, with a qualitative approach. She conducted a case study in a hospital that just started to look into the topic. Wu will conduct a second case study at a different hospital which has more experience with sustainable procurement, in order to compare the differences. Input from other WP’s are welcome!
“Will a supplier selection process also be taken into consideration?” asks someone in the audience. Wu: “Yes, defining a list of criteria that hospitals can use to select sustainable suppliers, is definitely part of the plan.”
Jacopo Parma (PhD TU Eindhoven) looks at business modeling perspective, how suppliers could change their business models. He will conduct several studies, the goals being to identify existing circular new business models (study 1), to design new circular ecosystems (study 2), to define a validated business model that reports examples to increase circularity in waste loops (study 3), and to demonstrate the effectiveness in real-world settings of the validated business models (study 4). The studies are expected to last until June 2028.
Workpackage 6 – How we engage and disseminate: dissemination of results of results and engagement in best practices with a larger audience
“It is important to make health professionals aware of why we have to move to circular hospitals”, emphasizes WP leader Ellen Bakker (Rotterdam University of Applied Science). Therefore we have to engage and disseminate knowledge.” The topic of sustainable health is not yet implemented sufficiently in the training program for nurses. WP6 members have written articles for publication in nursing journals, and are involved in the action group Sustainable Nurses. Furthermore, student assignments have been set up.


Kim Verhaegh (Leiden University of Applied Sciences) elaborates on the second goal of WP6: dissemination of evidence-based knowledge and best practices on national and international level. In order to achieve this, a collaborative network with several partners has been set up. The group will organize workshops and webinars and is actively involved in an online community where nurses can share knowledge/exchange experiences on implementing sustainable practices. The third aim of WP6 is to develop educational material for doctors and nurses. Especially the course material for nurses should focus more on how to implement the best practices and knowledge. WP6 has already written 2 articles and intends to do more research.
“Are nurses even allowed to change their behavior?” someone in the audience wonders. “There are so many rules.” “Nurses are trained to follow protocol”, Verhaegh agrees. “But we see a change coming. On a national level there is a program that stimulates a better leadership in nursing. Also, in the ‘green teams’ in the nursing departments a real change is happening.
Evaluation
Now that all workpackages have provided an update, it is time to evaluate this first edition of the Science Day: which points were helpful, was there anything missing? Comments/questions from the audience include:
- It is very useful, it makes it easier to reach out to each other;
- Maybe next year the partners (market, research organizations) can be involved;
- There are cross-overs between the packages, maybe next time we can present living labs with cross cutting themes instead of the separate workpackages;
- How do we compare with international initiatives?
Other suggestions are written on post-it notes. After taking a group picture, the Science Day comes to an end with a round of drinks.